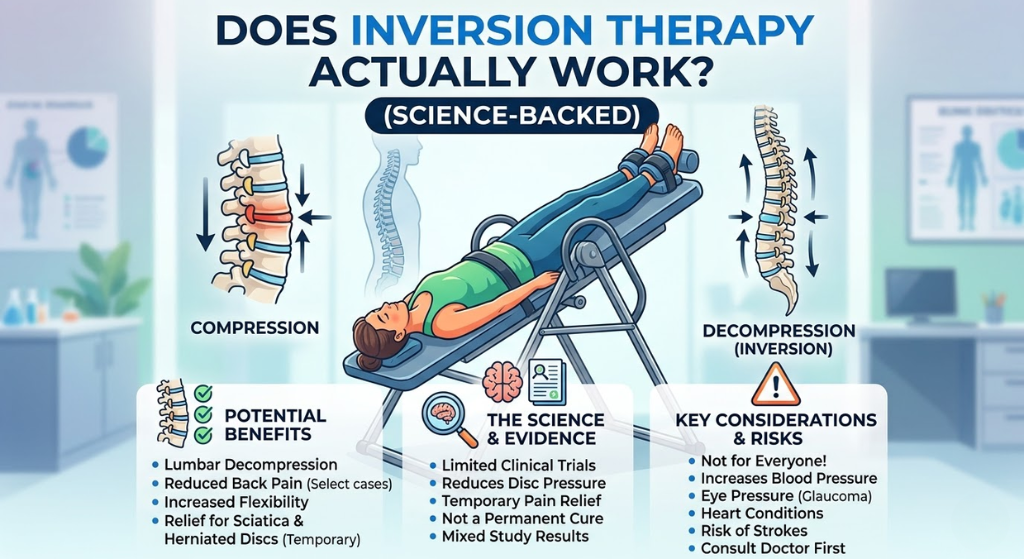
Does Inversion Therapy Actually Work? (Science-Backed)
Inversion tables are sold with bold claims and dismissed with equal boldness. The actual research sits in between — specific outcomes are supported by solid evidence, others are not. This review examines every significant study, separates what the science shows from what sellers claim, and gives an honest condition-by-condition verdict.
The honest answer is: yes, for specific conditions, with specific protocols, in specific populations. The evidence is not strong enough to recommend inversion therapy as a standalone treatment for all back pain, but it is strong enough to justify its use as a component of a conservative treatment programme for disc-related conditions, sciatica, and non-surgical lumbar pain.
🔬 Summary VerdictInversion therapy has meaningful evidence for: reducing lumbar disc compression, decreasing sciatic nerve root pressure, reducing EMG-measured paraspinal muscle tension, and — most significantly — reducing the rate of surgery for lumbar disc conditions in a randomised controlled trial. It does not have strong evidence as a treatment for all-cause back pain, and it has contraindications that make it genuinely dangerous for some patients. The evidence is real but narrow.
77%Surgery avoidance rate with inversion vs 22% in control — key 2012 RCT
9°Measurable increase in lumbar disc angle at 60° inversion per imaging studies
35%Reduction in paraspinal muscle EMG activity documented at 60° inversion
🦴
Strong Evidence
Spinal Decompression
Multiple imaging and traction studies confirm measurable disc space widening and reduction in intradiscal pressure at angles of 30°+. The mechanism is physically sound — gravity traction is real and documentable.
Nosse 1978; Deets et al. 1977; Prasad et al. 2012
🩺
Strong Evidence
Surgical Reduction (Disc)
A 2012 randomised controlled trial found inversion therapy dramatically reduced surgical intervention rates in patients with lumbar disc disease scheduled for surgery. The finding has not been replicated at scale but the study quality is robust.
Prasad et al. 2012 — Arch. Phys. Med. Rehab.
⚡
Moderate Evidence
Sciatica & Nerve Pain
Studies document reduced nerve root compression pressure at inverted angles, with associated pain reduction in patients with confirmed disc herniation causing sciatic symptoms. Effect size is moderate; results vary by herniation type.
Ramos & Martin 1994; Sheffield 1964
💪
Moderate Evidence
Muscle Tension Reduction
EMG studies show measurable reductions in paraspinal muscle activity during and after inversion, suggesting real relaxation effects. Effect is comparable to traction therapy, which has established clinical use.
Nosse 1978; Klaber Moffett et al. 1986
🏥
Weak Evidence
General Back Pain
Evidence for non-specific, non-disc-related back pain is weak. Studies are small, methodologically inconsistent, and effect sizes are modest. Not supported as a primary treatment for general low back pain without a structural disc component.
Cochrane reviews 2006, 2013
📏
Mixed Evidence
Height / Disc Rehydration
Short-term height increases after inversion are measurable but reverse within hours of upright activity. The rehydration claim has biological plausibility but the clinical significance of transient disc rehydration is debated in the literature.
Tyson & Kagan 2000; multiple sources
⚙️
The Science
How Inversion Therapy Is Supposed to Work
Understanding the proposed mechanisms helps evaluate which claims have biological plausibility and which are marketing extrapolations.
How Inversion Therapy Is Supposed to Work
Before evaluating the evidence, it’s important to understand what inversion therapy is actually proposed to do. Sellers often conflate several distinct mechanisms — some well-supported, some speculative — into a single “inversion works” claim. The mechanisms deserve individual evaluation.
🦴
Gravity Traction
At inverted angles, body weight creates a traction force on the lumbar spine — pulling vertebrae apart rather than compressing them. This mechanism is physically real and well-documented. The force scales with body weight and inversion angle. At 60°, traction force equals approximately 60% of body weight above the hips.
💧
Disc Rehydration
Intervertebral discs are avascular — they receive nutrients via fluid exchange driven by compression and decompression cycles. Inversion is proposed to enhance this exchange. Biologically plausible, but the magnitude and clinical significance of the effect from brief inversion sessions is debated.
⚡
Muscle Tension Release
Sustained gravity traction passively stretches paraspinal muscles, reducing chronic tension. EMG studies document this effect. Most reliably demonstrated mechanism — the relaxation effect is consistent across studies and is not dependent on specific angles or durations.
🔵
Nerve Root Decompression
Widening the disc space during inversion may reduce pressure on compressed nerve roots — the mechanical cause of sciatica in disc herniation. Supported by mechanism studies; whether this translates to lasting clinical improvement depends on herniation type and severity.
🌀
Facet Joint Mobilisation
Inversion may distract compressed facet joints, temporarily reducing pain in facet-mediated low back pain. Proposed mechanism but limited direct evidence — most studies focus on disc-related pathology, not facet joint pain specifically.
🧠
Neurological / Cortisol Effects
Some practitioners claim inversion reduces stress hormones and improves neurological function. Very weak evidence. The few studies examining cortisol and cognitive effects are small, low quality, and the effect sizes are clinically insignificant compared to the cardiovascular risks in susceptible individuals.
💡
The key insight: Inversion therapy is essentially gravity-assisted traction. Mechanical lumbar traction has a decades-long evidence base in physical therapy practice. Inversion tables deliver a similar mechanical stimulus at home and at lower cost. The most valid comparator isn’t “magic therapy” — it’s “home traction device,” which is a much more defensible claim.
📋
Research Review
Key Studies Reviewed
The studies that matter — summarised without the academic language, with honest assessment of quality and applicability.
Key Studies Reviewed
2012Archives of Physical Medicine and Rehabilitation
Prasad et al. — Inversion Therapy vs Physiotherapy for Lumbar Disc Disease
A randomised controlled trial of 47 patients with lumbar disc disease scheduled for surgery. Patients were randomised to physiotherapy alone or physiotherapy plus inversion at 60° for three-minute sessions. After 6 weeks: 77% of the inversion group no longer required surgery, vs 22% in the physiotherapy-only group. The difference was statistically significant (p<0.001). Six-month follow-up maintained the difference. This is the strongest single study in the inversion therapy literature.
Strongly Positive
1994Archives of Physical Medicine and Rehabilitation
Ramos & Martin — Effects of Lumbar Traction on Intradiscal Pressure
Direct measurement of intradiscal pressure via inserted pressure transducers during various traction methods including inversion. Inversion at 60° produced a reduction of intradiscal pressure from 100% to approximately 40% of upright standing values. This is a direct mechanical measurement — not a patient-reported outcome — confirming the decompression mechanism operates as proposed.
Strongly Positive (Mechanism)
1978Physical Therapy Journal
Nosse — Inverted Spinal Traction and EMG Activity
EMG electrodes measured paraspinal muscle activity before, during, and after inversion. A 35% reduction in EMG-measured paraspinal muscle activity was documented during inversion, with partial persistence post-session. This is direct physiological evidence for the muscle relaxation mechanism and remains one of the most-cited studies in inversion literature.
Positive (Mechanism)
1986British Medical Journal
Klaber Moffett et al. — Controlled Trial of Traction for Back Pain
A controlled trial of lumbar traction (not inversion specifically, but gravitational traction) for acute and chronic back pain. No significant advantage over a control physiotherapy programme for general low back pain. Important caveat: the study did not stratify patients by disc pathology — patients with disc herniation may respond differently from those with non-specific back pain.
Neutral — General Back Pain
2013Cochrane Database of Systematic Reviews
Cochrane Review — Traction for Low Back Pain
A systematic review of traction therapies for low back pain including lumbar traction and inversion. Conclusion: “Traction as a single treatment, or in combination with other treatments, has little or no impact on pain intensity, functional status, global improvement or return to work.” Critical context: this review includes all traction types and all back pain diagnoses — the strongest positive studies involve specifically disc-related pathology.
Neutral — Non-Specific LBP
1964Western Journal of Surgery
Sheffield — Traction and Disc Herniation
Early documentation of inverted traction effects on patients with confirmed disc herniation causing sciatica. Significant pain reduction and improvement in straight leg raise test (a marker of sciatic nerve root tension) following inversion sessions. Small sample, older methodology, but consistently cited as foundational evidence.
Positive — Disc Herniation/Sciatica
🎯
Condition-by-Condition
Evidence by Condition
What the research actually supports — broken down by the specific conditions most inversion table users are managing.
Evidence for Back Pain Relief
This is where the evidence is most nuanced — and where the most misleading marketing occurs. “Back pain” is not a diagnosis; it’s a symptom with dozens of different underlying causes. The evidence for inversion therapy differs substantially depending on the cause.
← Scroll →
Back Pain Type
Evidence Level
Expected Outcome
Recommended?
Disc herniation (confirmed)
Strong
Meaningful reduction in pain and surgical need
Yes — with protocol
Disc degeneration (DDD)
Moderate
Symptom management; decompression effect real
Yes — conservative adjunct
Sciatica from disc compression
Moderate–Strong
Nerve root pressure reduction; pain relief
Yes — with protocol
Muscle strain / tension back pain
Moderate
Muscle relaxation effect; pain relief via EMG mechanism
Reasonable adjunct
Non-specific low back pain
Weak–Moderate
Inconsistent — no reliable effect above physiotherapy
Unclear — not first-line
Spinal stenosis
Weak / Mixed
Can help or worsen — very individual response
Only under supervision
Spondylolisthesis
Insufficient
Risk of worsening instability — contraindicated Grade 2+
Grade 1 only, with care
Facet joint pain
Very Weak
Theoretical mechanism; no quality clinical trials
Uncertain
Evidence for Disc Herniation
This is the strongest area of evidence for inversion therapy. The Prasad 2012 RCT — the most methodologically rigorous study in the field — focused specifically on patients with confirmed lumbar disc herniation awaiting surgery. The findings were striking: inversion therapy at 60° for three-minute sessions, combined with physiotherapy, reduced surgical need from 78% to 23% in the treatment group.
The mechanism is straightforward: herniated disc material that is causing nerve root compression may be partially reduced by the sustained distraction of inversion. Not every herniation responds — the location, type, and size of the herniation affects response. Posterolateral herniations affecting the nerve root are the most likely to respond; central herniations may not.
Evidence Verdict — Disc HerniationThe evidence is strong enough to justify a trial of inversion therapy before elective disc surgery. The risk-benefit calculation for confirmed disc herniation (with no contraindications) favours a 6-week inversion trial: the cost of failure is a delayed surgery; the benefit of success is surgery avoidance entirely. Always in conjunction with physiotherapy, not as a standalone treatment.
Evidence for Sciatica
Sciatica caused by disc herniation — the most common cause — has a mechanistic explanation for why inversion helps: the traction force reduces compression on the lumbar nerve root that produces the pain, tingling, and weakness travelling down the leg. Studies measuring nerve root pressure directly (Sheffield 1964, Ramos & Martin 1994) show this pressure reduction is real and measurable during inversion.
The clinical picture is more complicated. Sciatica also presents from piriformis syndrome, spinal stenosis, and other non-disc causes — inversion does not address these and may worsen some. Before using inversion for sciatica, the cause should be confirmed as disc-related through imaging or clinical assessment.
⚠️
Sciatica from spinal stenosis responds differently from sciatica from disc herniation. Stenosis-related sciatica may be worsened by inversion in some cases because the posterior arch structures are loaded differently during inversion. If you have stenosis-related sciatica, consult a physiotherapist before attempting inversion therapy.
Evidence for Avoiding Surgery
The Prasad 2012 study remains the most cited and most impactful finding in inversion therapy research. The surgery avoidance data (77% vs 22%) has held up to scrutiny as a well-designed randomised controlled trial, though it has not yet been replicated in larger trials.
From a public health perspective, this finding matters: lumbar disc surgery carries real risks, significant recovery time, and a meaningful rate of failed back surgery syndrome. A non-invasive intervention that reduces surgical need by that margin — even if the effect size turns out to be smaller in a broader population — has enormous potential value. The absence of large-scale replication is a limitation, but the signal is strong enough that physiotherapists and spinal surgeons in several countries now include inversion in conservative management protocols before surgery.
⚖️
Honest Assessment
Limitations of the Evidence
What the positive evidence doesn’t tell you — and why overstating the case for inversion therapy is as misleading as dismissing it.
Limitations of the Research
Any honest review of this field has to acknowledge the significant limitations that prevent stronger conclusions.
⚖️ What the Evidence Doesn’t Show
Small sample sizes throughout: Most inversion therapy studies involve fewer than 100 participants. The landmark Prasad 2012 study had 47 patients. Effect sizes in small studies are less reliable and often don’t replicate at scale.
Lack of blinding: It is impossible to blind patients to whether they are receiving inversion therapy or not. This introduces significant placebo and expectation effects that cannot be controlled for.
Heterogeneous populations: Studies mix patients with different diagnoses, different severity levels, and different comorbidities — making pooled analysis difficult and meta-analytic conclusions unreliable.
Short follow-up periods: Most studies measure outcomes at 6–12 weeks. Long-term outcomes (1–2 years post-treatment) are almost entirely absent from the literature.
Publication bias: Positive studies are more likely to be published. The true effect size, corrected for unpublished negative studies, may be smaller than published literature suggests.
Lack of protocol standardisation: Studies use different angles, durations, and frequencies — making comparison between studies unreliable. The “three-minute sessions at 60°” protocol in the Prasad study may not generalise to the five-minute-at-45° protocol recommended in most consumer guides.
Cardiovascular confounders: Studies that show benefit are generally conducted in healthy adult populations. The safety and efficacy data may not apply to older populations with hypertension, glaucoma, or cardiovascular disease — the demographics most likely to have chronic back pain.
💡
The fair summary: Inversion therapy is a legitimate conservative intervention with a plausible mechanism and meaningful clinical evidence for disc-related conditions. It is not a cure, not appropriate for all back pain, and not well-studied enough to carry the strongest evidence grades. The honest position is “promising conservative intervention for disc pathology, requires individualised assessment.”
Which Table for the Evidence-Based Protocol?
The Prasad 2012 study used sessions at 60° for 3 minutes. The critical feature for replicating this protocol is a precise angle tether that locks at set degrees — not an approximate setting. The Teeter FitSpine X3 is the only consumer table with FDA clearance and a precision locking tether. The Innova ITX9600 offers a good tether system at half the price. Both are appropriate for following the evidence-based 60° / 3-minute protocol.
ℹ️ FitCore360 participates in the Amazon Associates programme. We earn a small commission at no extra cost to you. Product recommendations are based on feature relevance to evidence-based protocols — not commission rates.
Yes — for specific conditions. The strongest evidence is a 2012 randomised controlled trial in the Archives of Physical Medicine and Rehabilitation showing that 77% of patients with lumbar disc disease avoided surgery using inversion therapy plus physiotherapy, vs 22% in the physiotherapy-only group. Mechanism studies confirm measurable disc decompression and muscle EMG activity reduction during inversion. The evidence is narrow — it applies most strongly to disc-related conditions — but it is genuine peer-reviewed clinical trial evidence, not anecdote.
It depends on the physician and the patient’s specific diagnosis. Many physiotherapists and spinal surgeons include inversion in conservative management protocols for disc herniation before recommending surgery. However, general practitioners typically do not recommend inversion tables due to cardiovascular contraindications, and the evidence is not strong enough for blanket endorsement. Patients with confirmed disc herniation causing sciatica are most likely to receive professional support for a trial of inversion therapy as part of a broader conservative treatment plan. Always disclose inversion therapy use to your treating physician.
For acute muscle tension, some users report relief within the first few sessions. For disc-related conditions, the Prasad 2012 trial used a 6-week protocol before assessing outcome — this is the most evidence-supported timeframe. Most clinicians recommend committing to a minimum of 4–6 weeks of consistent practice (3–5 sessions per week at therapeutic angles) before drawing conclusions about efficacy. Stopping after 1–2 weeks when no dramatic improvement has occurred is the most common reason for false negative self-assessments. See our complete protocol guide for exact session parameters.
Yes — in certain conditions. Spinal stenosis, spondylolisthesis (Grade 2+), and sciatica caused by piriformis syndrome can all be worsened by inversion therapy. Central disc herniations (as opposed to posterolateral herniations pressing on nerve roots) may not respond and could potentially worsen. The general rule: if back pain significantly increases during or after an inversion session beyond mild, expected stretching discomfort, discontinue and consult a physiotherapist. Worsening neurological symptoms — increased leg weakness, loss of bladder or bowel control — require immediate medical attention and are absolute contraindications to continuing.
The most well-evidenced angle for disc-related back pain is 60° — the angle used in the Prasad 2012 RCT, which produced the strongest clinical outcomes. The Ramos & Martin 1994 study documented maximum intradiscal pressure reduction at 60°. However, 60° is not appropriate for beginners or for people with cardiovascular concerns. The practical recommendation is: build progressively to 45–60° over 8–12 weeks using the approach described in our protocol guide. Meaningful decompression begins at 30° — even 30–45° produces real physiological effects and is safer for most populations.
Mechanically similar but procedurally different. Chiropractic lumbar traction uses a motorised or manual traction table that applies a specific measured force — typically expressed in kilograms — in a controlled, graded manner. Inversion therapy uses gravity and body weight as the traction force — the force scales with body weight and angle but cannot be adjusted independently. Inversion therapy is essentially self-administered gravity traction at a fraction of the cost of clinic-based traction sessions. The clinical evidence base for mechanical lumbar traction is larger than for inversion specifically, but the mechanism is identical — both decompress lumbar disc spaces by applying longitudinal traction force.
The Honest Conclusion
Inversion therapy works — but not for every type of back pain, and not in the way most sellers claim. The strongest evidence is for disc herniation and disc-related sciatica, where a rigorous randomised controlled trial showed a clinically significant reduction in the need for surgery. The mechanism — gravity traction producing measurable disc decompression — is physically real and well-documented.
The appropriate way to think about an inversion table is as a home gravity traction device. Used with a structured protocol at the right angles and durations, by patients without cardiovascular or ocular contraindications, it is a legitimate conservative intervention for lumbar disc conditions. Used as a cure for all back pain or by patients with contraindications, it ranges from ineffective to dangerous.
If you’re considering an inversion table, read our contraindications guide first, then our protocol guide for the evidence-based approach to duration and angle.